


Patrocinados
Find Out How Upcoding in Medical Billing is Identified

In today’s healthcare environment, accuracy in documentation and coding plays a vital role in maintaining trust, compliance, and transparency across the medical system. One of the most critical compliance issues that organizations monitor closely is Upcoding in Medical Billing, a practice that can significantly distort patient records and create serious regulatory concerns. Understanding how this issue is identified is essential for maintaining ethical standards and ensuring proper reporting throughout the healthcare documentation process.
What Is Upcoding in Medical Billing?
Upcoding refers to the practice of assigning a higher-level medical code than what is actually supported by the patient’s diagnosis or treatment provided. Medical codes are designed to reflect the complexity, severity, and resources required for patient care. When these codes are intentionally or unintentionally inflated, it leads to inaccurate representation of medical services.
This issue can arise due to human error, misunderstanding of coding guidelines, or deliberate manipulation of records. Regardless of intent, upcoding disrupts the integrity of medical documentation and can trigger audits or compliance reviews.
Healthcare coding systems are structured with strict guidelines, meaning even small discrepancies in documentation can lead to incorrect code assignment. Because of this, identifying upcoding requires a combination of manual review, automated systems, and analytical techniques.
Why Identifying Upcoding Matters
Accurate medical coding ensures that patient records reflect true clinical conditions. When discrepancies occur, it can affect:
- Data reliability in healthcare systems
- Clinical decision-making
- Regulatory compliance
- Audit outcomes
Identifying upcoding is not just about preventing errors; it is also about maintaining the credibility of healthcare data. When records are accurate, healthcare providers, analysts, and policymakers can rely on them for meaningful insights.
How Upcoding in Medical Billing Is Identified
Detection of upcoding typically involves multiple layers of review. These layers work together to ensure accuracy and consistency in coding practices.
1. Clinical Documentation Review
One of the most effective methods of identifying upcoding is through detailed review of clinical documentation. Auditors compare medical records, physician notes, and treatment details with the assigned codes.
If the documentation does not support the complexity level of the code used, it raises a red flag. For example, if a simple consultation is coded as a highly complex service without supporting evidence, it may indicate upcoding.
Clear, thorough, and consistent documentation is essential for accurate coding validation.
2. Pattern Analysis in Coding Data
Another important method involves analyzing coding patterns over time. This includes reviewing:
- Frequency of high-level codes
- Comparison with similar cases
- Variations in coding across providers
When certain patterns deviate significantly from expected norms, it can signal potential inconsistencies. For example, if a provider consistently uses higher-level codes compared to peers handling similar cases, it may prompt further investigation.
Pattern analysis helps identify trends that may not be visible in individual cases but become clear when viewed across larger datasets.
3. Automated Coding Audits
Technology plays a growing role in identifying inconsistencies in medical coding. Automated systems can scan large volumes of data to detect anomalies based on predefined rules and benchmarks.
These systems flag cases where:
- Code levels appear unusually high
- Documentation is incomplete or mismatched
- Clinical details do not align with assigned codes
While automation cannot replace human judgment, it significantly enhances the speed and accuracy of initial detection.
4. Peer Comparison and Benchmarking
Benchmarking compares coding behavior against industry or departmental standards. This process helps identify outliers that may require further review.
If a provider’s coding patterns differ significantly from established benchmarks, it may suggest inconsistent coding practices. Peer comparison does not assume wrongdoing but serves as a tool for identifying areas that need closer evaluation.
This approach ensures fairness while still maintaining accountability within coding systems.
5. External and Internal Audits
Audits are one of the most direct methods used to identify upcoding. These audits may be conducted internally by compliance teams or externally by regulatory bodies.
During an audit, detailed records are reviewed to verify that assigned codes accurately reflect documented services. Auditors look for:
- Missing or incomplete documentation
- Inconsistencies between notes and codes
- Repeated use of high-complexity codes without justification
Audits are typically structured and systematic, ensuring that all relevant documentation is thoroughly evaluated.
Common Red Flags That Indicate Upcoding
Certain warning signs often prompt further investigation into coding practices:
Inconsistent Documentation
When clinical notes lack detail or fail to support the assigned code level, it raises questions about accuracy.
Repetitive High-Level Coding
Frequent use of high-complexity codes without variation may indicate a pattern worth reviewing.
Mismatch Between Diagnosis and Treatment
If the documented diagnosis does not align with the intensity of the coded service, discrepancies may exist.
Sudden Changes in Coding Behavior
A sharp increase in higher-level coding over a short period may signal the need for deeper analysis.
The Role of Training in Preventing Misidentification
Proper training for coding professionals is essential in reducing errors that could be mistaken for upcoding. When coders fully understand guidelines, documentation standards, and classification systems, the likelihood of incorrect coding decreases significantly.
Ongoing education helps ensure that coding practices remain consistent with evolving standards. It also reduces the risk of unintentional misinterpretation of clinical documentation.
Importance of Accurate Documentation Practices
Accurate and detailed documentation is the foundation of proper medical coding. Physicians and healthcare providers must ensure that all relevant clinical information is clearly recorded.
Good documentation supports:
- Correct code selection
- Smooth audit processes
- Reduced risk of discrepancies
When documentation is complete and precise, identifying errors becomes easier and more transparent.
Conclusion
Identifying upcoding is a multi-layered process that relies on careful review, data analysis, and consistent auditing practices. From clinical documentation checks to automated detection systems and peer benchmarking, each method plays a role in ensuring coding accuracy.
Patrocinados
Categorías
- Core Faith & Theology
- Christian Lifestyle & Practical Living
- Community & Church Life
- Creative & Inspirational Content
- Cultural Engagement & Outreach
- Practical Ministry & Resources
- Niche & Specialized Blogs
- Seasonal & Themed Content
- Interactive & Community-Driven Content
- Humor & Relatable Content
- Other
Read More
We provide professional solutions designed to protect properties through reliable gutter maintenance and tree care. Our services focus on preventing structural damage, improving drainage efficiency, and enhancing outdoor spaces. With a skilled team and advanced tools, we ensure every project is completed with precision and long-lasting results using First Choice Gutter Cleaning Sydney...

Even noodle boxes are considered a significant constituent of the modern food packaging and it makes such a simple task serving noodles look like a feast. Whether it is a restaurant, food truck, or catering, the correct packaging may turn out to be beneficial to the brand, retain the food quality,y and increase customer satisfaction. These containers are utilitarian yet attractive...

Moving into a new home is an exciting milestone, but it also comes with many responsibilities. One of the most essential tasks is ensuring the property is clean and sanitized. Move-in Cleaning near me helps homeowners settle into a fresh and safe environment. This process ensures that every corner of the new home is free from dust, dirt, and allergens, creating a comfortable living space from...

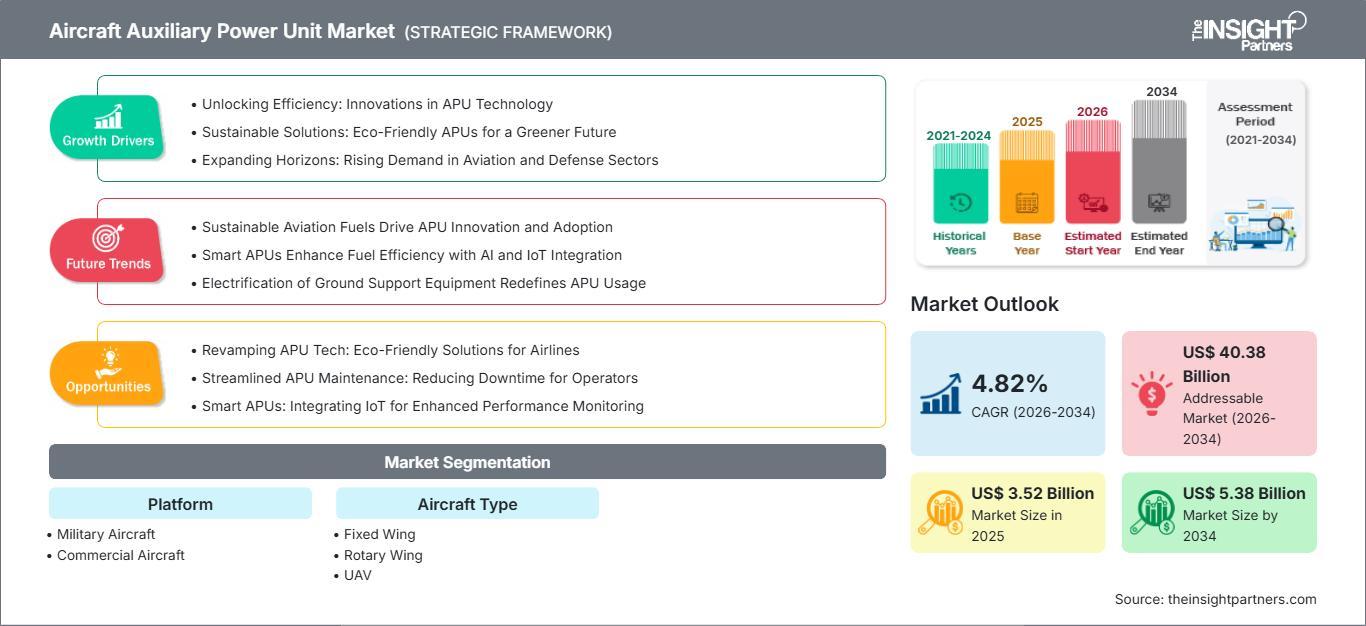
The Aircraft Auxiliary Power Unit (APU) Market is experiencing steady growth as airlines, aircraft manufacturers, and defense organizations continue to focus on operational efficiency, fuel optimization, and enhanced onboard power capabilities. Auxiliary power units play a crucial role in modern aircraft by providing electrical power and pneumatic energy when the main engines are not operating....
Advanced Driver Assistance Systems Calibration Equipment Market Summary: According to the latest report published by Data Bridge Market Research, the Advanced Driver Assistance Systems Calibration Equipment Market CAGR Value The global advanced driver assistance systems calibration equipment market size was valued at USD 392.54 million in 2024 and is expected to...
